
Mini Pig Sickness and Diseases: What Should You Be Looking For?
Mini Pig Health
Pigs can have a variety of illnesses or diseases. The most common illnesses are going to be discussed on the following pages. If your pig has a temperature, is lethargic, not eating or drinking, you need to take your pig to the vet. You can ask people online what is going on with your pig, but it can really turn into an emergency very fast. Is waiting for others to respond worth your pigs life? No, it's not. Fever above 103, a pig that isn't eating or drinking, a pig that is usually playful doesn't want to get up, a pig that is having seizures or developing sores, all these symptoms need to be treated by a veterinarian. Do NOT waste your time asking someone who may or may not even be knowledgable what you should do. This may make the difference in life or death for your pig. Pigs tend to mask any illness they're experiencing until they're no longer able to hide it. You may only see subtle signs in the beginning such as a change in behavior or maybe your pig is resting more than usual. This may not be anything, but, it could be the first warning signs of something internal going on. Pay attention, keep a pig journal so you can remember what is normal and what is not. You will be the first person to notice a change in your pig, no one will know your pig better than you. Stay proactive and always investigate further if you think something is wrong.
We have tried to collect as much information as possible in addition to as many pictures as possible to demonstrate serious ways a pig may present or the varying ways to prevent or treat each illness. Some of these illnesses are more common than others and we have focused the efforts on diseases we have seen pigs within our pig community diagnosed with. Although some diseases affect the skin, they're listed here because they're an illness/disease. There is a skin problem link as well that will address more common skin issues. As we get the website up and running, we will add to it and create additional pages and documents as the need arises. Please don'e hesitate to email us directly if you'd like to see a topic discussed here. [email protected]
Sometimes diagnostic testing is required to determine what organisms is affecting your pig. These samples can come from a variety of locations including blood, nasal swabs, tissue samples, oral fluids, tonsil scrapings and tracheobronchial swabs, bronchoalveolar lavage fluid, cervical swabs, semen, and urine and the feces. These are just a few of the tests that can isolate the organism so your vet can treat it effectively and efficiently. Other tests include imaging of some kind in addition to a hands-on exam by a veterinarian.
To control infectious disease it is helpful to understand how organisms are disseminated and gain access to the pig. Each organism has individual properties that determine how long it will survive outside the pig, how infective it is, and how easily it is transmitted. The methods by which disease spreads include the following:
Please click on the illness that you'd like more information about and it will take you to that page.
Erysipelas
Leptospirosis
Brucellosis
Salt Toxicity
Mysterious Head Tilt
Pneumonia/Swine flu
Gastric Ulcers
Gastrointestional disorders
Dippity Pig Syndrome
Swine Pox
Foot & Mouth Disease
Pseudorabies
Mycoplasma Hyosynoviae
Seizures
Salmonellosis
Obstructions
PSS (porcine stress syndrome)
Urinary Blockages
Arthritis
Artophic Rhinitis
Heart Disease/Defect
Why is my pig coughing?
Pasteurellosis
UTI's in pigs
Rabies and pigs
Cancer and pigs
Uncommon illnesses
Toxoplasmosis
Melioidosis
Coccidiosis
Common Skin Issues
Dry Skin
Abscesses
General Lumps and Bumps
Another section on our website is about first aid. Click on the topic you wish to learn more about to take you to that page. The main page for first aid has a list of items that are helpful to have on hand in case of emergencies. You can see that page by clicking here.
Constipation
Salt Toxicity/Water Derivation
Diarrhea
Vomiting
Fever
Pig gorges on food
Basic wound care
Shock and pigs
Fractures and pigs
Paralysis
Emergency supplies to have on hand/basic first aid info
Disease pathology guide written by University of Iowa. GREAT information and pathology pictures discussing congenital defects as well as common diseases. This downloadable document shows you what is going on internally with your pig when diagnosed with any of the diseases/illnesses referenced in this article.
We have tried to collect as much information as possible in addition to as many pictures as possible to demonstrate serious ways a pig may present or the varying ways to prevent or treat each illness. Some of these illnesses are more common than others and we have focused the efforts on diseases we have seen pigs within our pig community diagnosed with. Although some diseases affect the skin, they're listed here because they're an illness/disease. There is a skin problem link as well that will address more common skin issues. As we get the website up and running, we will add to it and create additional pages and documents as the need arises. Please don'e hesitate to email us directly if you'd like to see a topic discussed here. [email protected]
Sometimes diagnostic testing is required to determine what organisms is affecting your pig. These samples can come from a variety of locations including blood, nasal swabs, tissue samples, oral fluids, tonsil scrapings and tracheobronchial swabs, bronchoalveolar lavage fluid, cervical swabs, semen, and urine and the feces. These are just a few of the tests that can isolate the organism so your vet can treat it effectively and efficiently. Other tests include imaging of some kind in addition to a hands-on exam by a veterinarian.
To control infectious disease it is helpful to understand how organisms are disseminated and gain access to the pig. Each organism has individual properties that determine how long it will survive outside the pig, how infective it is, and how easily it is transmitted. The methods by which disease spreads include the following:
- Direct contact with the infected pigs, including newly purchased/rescued pigs.
- Mechanical dissemination by vehicles, particularly pig transporters.
- Mechanically by on farm equipment, boots and clothing.
- Infection transmitted by people (e.g. influenza).
- Movement of birds, rats, mice, flies, dogs, cats and wildlife (e.g. wild boars).
- Environmental contamination on the pig farm (e.g. moving pigs into a contaminated pen, movement of contaminated feces along defecating passages).
- Contaminated food and water.
- Airborne transmission in aerosol droplets or dirt.
- Biting insects (e.g. eperythrozoonosis).
Please click on the illness that you'd like more information about and it will take you to that page.
Erysipelas
Leptospirosis
Brucellosis
Salt Toxicity
Mysterious Head Tilt
Pneumonia/Swine flu
Gastric Ulcers
Gastrointestional disorders
Dippity Pig Syndrome
Swine Pox
Foot & Mouth Disease
Pseudorabies
Mycoplasma Hyosynoviae
Seizures
Salmonellosis
Obstructions
PSS (porcine stress syndrome)
Urinary Blockages
Arthritis
Artophic Rhinitis
Heart Disease/Defect
Why is my pig coughing?
Pasteurellosis
UTI's in pigs
Rabies and pigs
Cancer and pigs
Uncommon illnesses
Toxoplasmosis
Melioidosis
Coccidiosis
Common Skin Issues
Dry Skin
Abscesses
General Lumps and Bumps
Another section on our website is about first aid. Click on the topic you wish to learn more about to take you to that page. The main page for first aid has a list of items that are helpful to have on hand in case of emergencies. You can see that page by clicking here.
Constipation
Salt Toxicity/Water Derivation
Diarrhea
Vomiting
Fever
Pig gorges on food
Basic wound care
Shock and pigs
Fractures and pigs
Paralysis
Emergency supplies to have on hand/basic first aid info
Disease pathology guide written by University of Iowa. GREAT information and pathology pictures discussing congenital defects as well as common diseases. This downloadable document shows you what is going on internally with your pig when diagnosed with any of the diseases/illnesses referenced in this article.
| disease_guide.pdf |
What Are Signs Of Illness In Mini Pigs?
Basic signs your pig may be sick?
- No desire to eat or drink. Not rising to eat and/or drink.
- Lethargic (no energy, just wants to lay around).
- Fever (over 101 is considered to be feverish for "most" pigs).
- Lameness.
- Behavioral changes. A normally friendly pig can become reclusive, start doing unusual things, potty in the wrong spot, become aggressive, etc. YOU will be the first to notice subtle behavioral changes.
- Changes to the skin, perhaps lesions or sores developing.
- Difficulty urinating or defecating. (peeing/pooping)
How Sick Is Your Pig?
Severity of illnesses will decide the treatment plan. Some diseases are too far along for any kind of curative treatment and pallative care can sometimes be initiated. Unfortunately, in some of these more severe cases, euthanasia is the only humane solution. If you feel like this is not the case, PLEASE take your pig to someone else for a second opinion or call another well respected vet to get their perspective. There have been times when an inexperienced vet simply didn't know what was available to help or treat a pig and a 2nd opinion could've saved a pig's life.
Common Pig Problems Based On Body System
Gastrointestinal System
Gastritis and gastric foreign bodies are common in PBPs because they are omnivorous and prone to ingest many types of objects. Keeping PBPs indoors where they are unable to root and restricting calorie intake to prevent obesity probably contribute to this continual search for food. Dividing the daily ration into two or more portions and furnishing low-calorie foods (eg, lettuce, cabbage, celery, carrots, or green grasses) may help satisfy appetite. If an ingested foreign body is small or pliable enough, it may pass through the GI tract and cause mild gastritis that is self-limiting or only requires antibiotic therapy. Larger objects may remain in the stomach or partially pass into the duodenum or a more distal part of the small intestine. Clinical signs such as vomiting and colic can be acute but may be more subtle and increase in intensity over several days or weeks. Radiographs may reveal obvious foreign material or delayed gastric emptying. CBCs may indicate infection but are usually not informative; serum enzyme and electrolyte panels may only reflect dehydration. Surgical correction is indicated but may not be successful if extensive necrosis of GI tissue is present. Fluid replacement and nutritional supplementation plus antibacterial therapy and tetanus prophylaxis are indicated in convalescing PBPs
Lower GI obstruction due to bowel stricture occurs in geriatric PBPs. Anorexia, scant fecal production, and a bloated abdomen with massively distended intestines seen radiographically are typical. Sedation and endoscopic examination of the oral cavity, esophagus, and stomach are indicated to exclude other problems. Exploratory laparotomy and anastomosis with or without bowel resection is usually remedial.
1. Colibacillosis or Escherichia coli diarrhea is generally an important disease in young PBPs. Mortality may be high in piglets that have not ingested adequate colostrum in their first 24 hr of life. Older PBPs apparently develop resistance to colibacillosis. Diagnosis is through signalment, history, and fecal culture. Sanitation to minimize infective doses of pathogenic coliforms in the environment of young, nursing PBPs is important for prevention. Commercial swine vaccines to prevent colibacillosis are available but must be given to sows before farrowing to stimulate immunity and secretion of IgA into the milk. Treatment is based on in vitro antibacterial sensitivity testing, but antibiotics such as oral or injectable gentamicin or injectable ceftiofur are usually effective
2. Enterocolitis from Salmonella typhimurium infection can affect PBPs of any age, but it usually occurs after weaning. Sources of salmonellae include waste food from overturned garbage cans, exposure to carrier swine (such as the dam), or fecal material from other animal species. Mild to severe diarrhea with mucus and blood can result. Diagnosis is through signalment, history, and fecal culture or PCR. Salmonella spp are characteristically resistant to many antibiotics, so in vitro antibacterial sensitivity testing is important. Parenteral gentamicin at 2.2 mg/kg/day for 3 days may be effective in the interim. Untreated PBPs may die. Some recovered PBPs may develop rectal stricture after enterocolitis, resulting in megacolon and a distended abdomen. Subsequent straining to defecate can cause rectal prolapse. Surgical correction of the rectal prolapse will not correct the underlying problem. Owners should be advised that many Salmonella spp, including S typhimurium, are zoonotic. Healthy PBPs may be tested via fecal culture or PCR to determine their salmonella status. Multiple tests are more accurate predictors than single tests. Vaccines available for commercial swine have not been used much in PBPs.
Bacteremia or septicemia after S choleraesuis infection may also affect PBPs, usually after weaning. Sources of infection are similar to those of S typhimurium. Mild to inapparent diarrhea followed by fever, lethargy, anorexia, cyanosis of extremities, recumbency, and death may ensue. Diagnosis, treatment, prevention, and zoonotic potential are similar to those of S typhimurium; zoonosis is mainly a threat in immunocompromised people.
3. Constipation may be seen in PBPs; however, each normal bowel movement of a PBP is typically composed of one or more cylindrical formations made up of smaller, multiple fecal balls that may give the impression that the PBP is constipated. True constipation may occur due to low water intake in sedentary PBPs or to an actual disease. Careful evaluation is warranted before treatment is administered. Enemas may be contraindicated if there is pathology such as colitis. In simple constipation, fecal softeners or mild laxatives such as sodium sulfate or magnesium sulfate may be used. These should be given with food, if possible, because forced PO (by mouth) administration can result in aspiration pneumonia and death, especially with mineral oil. Encouraging increased water intake by flavoring with fruit juice or liquid gelatin may be helpful. Regular exercise is also beneficial to promote normal feces.
4. Rectal Prolapse This is a painful condition in which one or more layers of the rectum protrude through the anus. The prolapse may involve only one rectal membrane (incomplete) or all the layers of the rectum (complete). The condition is most frequently associated with a prolonged but ineffectual effort to empty the rectum. It is most common in young animals with severe diarrhea and some other lower intestinal tract conditions. Eating foreign objects may trigger this condition. Straining to urinate can also be accompanied by rectal prolapse, so obtaining a correct diagnosis is important. Your veterinarian can treat this condition surgically, and recovery is considered routine. Once your pig has had a rectal prolapse, the chances of it happening again are greater.
Rectal prolapse occurs due to straining from bowel irritation from diarrheal disease, rectal stricture after S typhimurium enterocolitis or previous rectal prolapse repair, cystitis or urolithiasis, persistent coughing, dystocia, or possibly genetic predisposition. Small, uncomplicated, recent rectal prolapses may be repaired via anesthesia and purse-string closure of the rectum that allows for minimal passage of feces. Larger, complicated prolapses require surgical excision. Recurrence is less likely after surgery but is possible regardless of method of repair.
5. Salmonella Infections Enterocolitis is an infection often caused by Salmonella typhimurium bacteria. Pigs can be infected at any age, but after weaning is most common. Sources of infection include waste food from overturned garbage cans, exposure to other pigs with the infection, and wastes from other animals. The signs include mild to severe diarrhea with mucus and blood showing in the fecal matter. Fever, lethargy or weakness, and a bluish or purplish discoloration of the legs, ears, and jowls may also occur. Diagnosis is made by testing your pig's feces for the bacteria. At the same time, your veterinarian will test the bacteria to determine which medication can best treat your pet's infection. Untreated pigs may die from the infection, so prompt veterinary treatment is important.
Salmonella choleraesuis bacteria may also cause infection. The signs are similar to those of S. typhimurium infection, described above. Again, early veterinary intervention and treatment is important as this infection can cause death.
All Salmonella infections should be treated carefully because the bacteria can easily infect humans. Be sure to wash hands carefully and thoroughly with a strong soap, especially when disposing of waste materials. Children should not be exposed to pigs with any Salmonella infection as they can easily be infected.
Integumentary System
1. Dry, flaky skin with minimal to severe pruritus is seen in virtually all PBPs. Wiping down the skin with wet towels each week will remove the flakes. Moisturizing lotions (eg, aloe vera) also temporarily alleviates this problem. Fatty acid supplementation can be used as a more longterm remedy, but caution must be exercised not to promote obesity.
2. Sarcoptic mange is the most important ectoparasitic disease of PBPs. Intense pruritus and dermatitis are the basis for a presumptive diagnosis. In many cases, the owners have pruritic skin lesions on the arms or abdomen. Examination of skin scrapings (deep enough to contain some blood) from several sites usually confirms the diagnosis in advanced cases but may be negative in less advanced cases if very few mites are present. In young PBPs, the source of infestation is usually the dam; in older PBPs, the source is usually other infested pigs. Young PBPs isolated from other pigs and kept as pets may harbor mange mites as a subclinical problem until mite populations increase sufficiently to make the condition obvious. Treatment with ivermectin (300 mcg/kg, SC, repeated in 2 wk) or doramectin (300 mcg/kg, IM, repeated in 3 wk), is indicated. Recently acquired young PBPs should be given a routine preventive injection of either parasiticide when first presented for examination.
3. Melanoma is an important skin tumor in swine. Tumor removal and evaluation of metastatic potential through histopathology is important for prognosis. Spontaneous regression of melanomas, with subsequent depigmentation of the hair, skin, and iris, is occasionally seen in PBPs; affected swine usually have normal life spans.
4. Sunburn may develop in PBPs exposed to sudden, high-intensity sunlight. Skin lesions may or may not be obvious, but affected PBPs appear painful and seem to have hindlimb weakness or paresis. A sunburned PBP may be “down in the back legs” and show intense pain with vocalization. A thorough history is important for the diagnosis. Exposure to further sunlight should be prevented. Symptomatic treatment is remedial.
5. Bleeding back syndrome (dippity pig syndrome) is of unknown etiology. Signs are almost identical to those of sunburn (pigs dip their backs, vocalize, and show signs of extreme pain) but with no history of sun exposure. Circular, serum-oozing lesions of various sizes are seen on lumbar skin surfaces. Affected PBPs recover in several days with restricted activity with or without symptomatic treatment. The condition may recur in some animals.
6. Erysipelas is an infectious disease caused by Erysipelothrix rhusiopathiae and is one of the oldest known diseases that affect growing and adult swine. Up to 50% of pigs in intensive swine production areas are considered to be colonized with E rhusiopathiae. The organism commonly resides in the tonsillar tissue; nonpathogenic species (E tonsillarum) have been described as residing in the tonsillar tissue also.
Disease outbreaks may be acute or chronic, and clinically inapparent infections are believed to occur. Acute outbreaks are characterized by sudden and unexpected deaths, febrile episodes, painful joints, and skin lesions that vary from generalized cyanosis to the often-described diamond skin (rhomboid urticaria) lesions. Chronic erysipelas tends to follow acute outbreaks and is characterized by low mortality, enlarged joints, lameness, and postmortem evidence of vegetative endocarditis. Pigs with valvular lesions may exhibit few clinical signs; however, when exerted physically they may show signs of respiratory distress and possibly succumb to the infection. (Please see the common disease section for additional information about Erysipelas)
(source: http://www.merckmanuals.com)
Musculoskeletal System
1. Lameness due to lower back, hindlimb, or forelimb weakness is common in PBPs. Because of their conformation, PBPs are susceptible to muscle pulls, ligament damage, and fractures of the back and limbs. Because PBPs usually struggle against manual restraint (predisposing to injury), sedation or anesthesia is often used for procedures such as prolonged examination, radiography, foot trimming, blood collection, and dental work. Tiletamine-zolazepam at 2.2 mg/kg body weight, IM (in the ham), provides excellent analgesia and chemical restraint for these minor procedures; recovery, although smooth, is prolonged and requires careful monitoring. Gas anesthesia is also used and has the advantage of rapid recovery time. Fasting for 24 hr and withholding water for 4–6 hr before sedation or anesthesia is recommended.
PBPs with injuries to the back or limbs are usually treated with anti-inflammatory drugs, such as buffered aspirin with antacid, flunixin meglumine, or glucocorticoids (eg, dexamethasone). Polysulfated glycosaminoglycan and/or glucosamine/chondroitin sulfate products may be tried in nonresponsive cases.
Fractures of the distal humerus and elbow area and femur are common. These occur from jumps off furniture (distal humerus), dog bites (elbow area), restraint (elbow area and femur), equine kicks (femur), and other trauma. Repair via pins, screws, plates, and external devices successfully restores some range of motion if fractures are immobilized properly and any sepsis is controlled
2. Infectious arthritis may affect the very young to older PBPs. Lameness with or without joint swelling in one or more limbs is the usual clinical finding. Erysipelothrix rhusiopathiae, Streptococcus spp, Mycoplasma hyosynoviae, M hyorhinis, Staphylococcus spp, and Haemophilus parasuis are possible causes. Treatment early in the disease course with an effective antimicrobial (eg, lincomycin at 11 mg/kg, bid for 3 days) may be effective. Treatment after chronic changes have occurred, antimicrobial ineffectiveness against the etiologic agent, or misdiagnosis are reasons for treatment failure and persistence of lameness. In chronic cases, pain management with anti-inflammatory drugs should be considered. Polyarthritis from neonatal infection of the navel may be due to various environmental bacteria, including Pseudomonas spp. If degenerative arthritis and joint fusion from chronic inflammation are present after polyarthritis, euthanasia may be warranted. Osteochondrosis may also be considered in shoulder, elbow, hip, and stifle lameness, but this condition is not common in slow-growing, light-muscled animals such as PBPs.
3. Overgrown and/or cracked hooves are a common cause of lameness. Regular exercise on abrasive surfaces (eg, concrete) will wear hoof ends and help keep them the appropriate length. In PBPs with overgrown, elongated hooves, normal yearly length can be maintained by routine yearly trimming under sedation or anesthesia. Hoof cracks can be caused by overgrown hooves. PBPs with cracked hooves may additionally require antiseptic cleaning with tamed iodine and systemic antimicrobial therapy (ceftiofur at 4.4 mg/kg/day for 3–10 days, or ampicillin at 11 mg/kg, PO, bid for 7–10 days).
4. Zygomycosis from Mucor spp infection has occurred in the distal hindlimb of a PBP. The large growth that encompassed the entire foot was composed of infected/abscessed tissue that involved bone. Amputation was remedial.
5. Tetanus may occur after wound contamination from dog bites, skin abrasions, oral cavity abrasions, or surgical procedures. Tetanus toxoid should be part of the routine vaccination schedule of PBPs at high risk of exposure. If there is no current tetanus toxoid vaccination, tetanus antitoxin (500–1,500 U, depending on body weight) should be administered IM in the neck after recovery from any surgery or dental procedure (eg, trimming of canine teeth). Treatment for tetanus is by massive doses of tetanus antitoxin and penicillin early in the disease, along with tranquilizers, isolation to minimize external stimuli, and supportive therapy.
6. Fractures Breaks in leg bones and back bones are common in potbellied pigs and require surgery. Implanted pins, screws, plates, and other devices can help restore motion and strengthen the affected bone(s). Providing an environment that does not encourage your pig to jump on furniture or higher surfaces is the best way to reduce the chance of broken bones. Stairs are a challenge for pigs, and providing ramps between the levels in your home is a good way to solve this problem. Please don't let your pig jump off of furniture, as this can lead to these kind of fractures.
Nervous System
1. Systemic bacterial infection can be caused by (in approximate decreasing order of importance) Streptococcus suis type 2, other Streptococcus spp, Salmonella choleraesuis, Haemophilus parasuis,Escherichia coli, other gram-negative bacteria, and Listeria monocytogenes. CNS signs may include fever, depression, incoordination, staggering, postural abnormality, head tilt, circling, nystagmus, seizures, and death. PBPs are most commonly affected from birth through 4–6 mo of age. Treatment with the appropriate antibacterial therapy (eg, extra-label florfenicol, which penetrates the blood/brain barrier) in the early stages of infection is most effective; however, death may be the first clinical sign. Because S suis type 2 is a zoonotic disease agent, care should be exercised to prevent human infection when performing necropsies on pigs dying from suspected CNS disease.
2. Overheated PBPs may be depressed, inactive, and recumbent and show open-mouth breathing or panting with an initial fever followed by a subnormal and decreasing temperature. The prognosis is grave, but some overheated PBPs may respond to resting on a cool surface and cooling only the head with water for 10–15 min followed by packing ice bags around the head. If the temperature is still not controlled, cold-water enemas can be used while additional areas of the skin surface are packed in ice. Symptomatic treatment is continued as indicated. You can try ice packs in the groin area and alcohol applied to the hooves. Wet wraps around the legs and cool wet cloths around the neck help as well.
3. Salt toxicity occurs after water deprivation for extended periods of time followed by sudden rehydration or, less commonly, after prolonged consumption of high-salt foods. Affected PBPs may have seizures, walk aimlessly, or show other CNS signs such as blindness or postural abnormalities. Diagnosis in the affected live animal is confirmed by high levels of serum sodium, usually 160–183 mEq/dL (normal range 142–153 mEq/dL). Gradual rehydration and symptomatic treatment to counteract cerebral edema is indicated, but severely affected PBPs may only be stabilized to a vegetative and blind status. The histopathologic finding of eosinophilic infiltration into brain tissue is also diagnostic.
4. Seizure from unknown cause occurs in PBPs.
Respiratory System
1. Atrophic Rhinitis This infectious disease of younger pigs initially causes sneezing, a runny or bloody nose, tearing, and distortion of the nose or snout. It is most often caused by Bordetella bronchiseptica and/or Pasteurella multocida, and less commonly by cytomegalovirus. It is usually transmitted from the mother to the piglet before weaning but can be transmitted from pig to pig after weaning. The more severe the rhinitis, the more likely it is that the pig's nose or snout will be permanently distorted. This distortion may become more pronounced as the pig grows.
Bleeding from the nose, with or without a crooked snout, is a common sign of the disease. Early treatment with antibiotics is recommended for acute cases. For pigs with chronic nose bleeds, cooling the area with cold water and keeping the pig calm are helpful. For pigs in dry climates, increasing the humidity of the air can offer some relief. Vaccines are available for atrophic rhinitis, but they must be used in pregnant mothers and unweaned pigs to be most effective. Watch newborn piglets for sneezing, nasal discharge, and tears. If these signs appear, your veterinarian should be consulted for prompt treatment.
2. Pneumonia can be a very serious disease in PBPs because of their relatively small lung capacity. The most common cause of pneumonia is from initial Mycoplasma hyopneumoniae infection, which immunocompromises the lungs, followed by Pasteurella multocida infection. Young pigs contract these infectious agents from their dams or from mixing with infected pigs after weaning. Antibiotic treatment may be more effective if directed against P multocida, because this bacterium becomes the most important pathogen once coughing is present for several days. Vaccines available for M hyopneumoniae in domestic commercial swine have been used in young PBPs to prevent mycoplasmal pneumonia and subsequent Pasteurella pneumonia. Vaccination in older PBPs is probably unnecessary unless risk of exposure warrants continued use.
Actinobacillus pleuropneumoniae causes a life-threatening pneumonia that may occur after infection from the sow or exposure to carrier animals. Signs range from coughing, fever, and lethargy to sudden death, depending on the serotype of A pleuropneumoniae. Prompt antibiotic treatment with penicillin or ceftiofur is indicated. Recovered PBPs usually have permanent tissue loss in affected lung areas and may have recurrent respiratory problems. Vaccines available for domestic commercial swine may be used in PBPs if there is an exposure risk.
3. Swine influenza (see Swine Influenza) is an important viral pneumonia in PBPs that are taken to fairs, exhibitions, and petting zoos and exposed to other pig populations. It is usually self-limiting after 7–10 days but can be fatal. H1N1, H3N2, H1N2, and H2N3 are the most common strains in domestic swine. Multivalent vaccines available for domestic swine could be used in PBPs if indicated. Swine influenza is a zoonotic disease.
Urinary System
1. Cystitis and urolithiasis are common in PBPs. Signs include frequent urination or straining to urinate. Urinalysis, urine culture, CBC, serum chemistry, radiography, and ultrasonography are important diagnostic aids. A sterile urine sample for culture can be obtained via cystocentesis. Cystitis without triple phosphate crystalluria should respond to extended antibacterial therapy based on in vitro sensitivity testing. Acidification of the urine may minimize recurrence of infection. Nephritis can occur after cystitis as an ascending infection. Leptospirosis may be a primary cause of nephritis. Increased BUN and creatinine values may aid in the diagnosis of nephritis and kidney failure. A 6-way vaccine for leptospirosis is routinely given to breeding PBPs (see Vaccinations) but may also be considered for routine use in rescue operations where many PBPs are housed in close contact. Vaccination may possibly reduce renal shedding of leptospires should PBPs become chronically infected and, therefore, minimize transmission of this zoonotic disease.
In a PBP that is straining and unable to urinate, the bladder size should be reduced immediately by cystocentesis after sedation and radiography (plain or contrast) or ultrasonography to evaluate the location of urethral and bladder stones. If the blockage is in the urethra, cystotomy is recommended (both sexes) to identify and remove calculi in all possible locations. Calculi in the urethra of males may be removed by cutting through the sheath to expose the distal penis, catheterizing the urethra, and backflushing into the bladder. Calculi that cannot be removed by this method must be surgically removed by incising the urethra at the location of the blockage. However, scar tissue at the healed incision may also cause urethral obstruction. Suturing of the urethra is followed by cystotomy and bladder flushing to minimize recurrence and then by inspection for more calculi. The bladder is then closed, and a Foley catheter is inserted into the bladder, tunneled through the abdominal muscles, and sutured to the skin. Several days later, the Foley catheter is occluded, and the urethra is inspected to determine patency and urine flow; if not patent, the Foley catheter is opened again, and the process is repeated several days later. When the urethra becomes patent, the Foley catheter is removed. Although the urethra in females is short, blockage can still occur. Because urethral catheterization is difficult without endoscopy, a Foley catheter is inserted into the vagina and inflated, and a purse-string suture is placed at the vulva. Retrograde flushing through the urethral opening in the vaginal floor is attempted. A cystotomy is then performed to remove all possible calculi, followed by routine closure of the bladder. Foley catheter placement into the bladder may not be necessary. Further treatment includes antibiotic therapy and acidification of the urine. Despite these efforts, some affected PBPs do not recover and require euthanasia. Perineal urethrostomies are usually only temporarily successful because the surgical site becomes occluded by amorphous material or urethral polyps, and patency cannot be reestablished. However, surgical methods have been described to correct failed perineal urethrostomies in PBPs. Rupture of the bladder is a grave complication because normal bladder tone may not return even after stones have been removed and the bladder has been surgically repaired. Laser lithotripsy has been used to fracture urethral calculi not removable by flushing.
2. Psychogenic water consumption should be considered in PBPs (especially young PBPs) with polydipsia and polyuria. PBPs may develop a habit of drinking water and urinating frequently because of possible boredom or unknown causes. Cystitis and crystalluria should be eliminated as differential diagnoses. Measuring urine specific gravity before and after a 12-hr water fast will demonstrate whether the affected PBP is able to concentrate urine. Ability to concentrate urine indicates normal kidney function and helps exclude diabetes insipidus. Estimating the daily water intake and urine output will further aid the diagnosis of psychogenic water intake or establish that water consumption and urination are, in fact, normal. Relieving boredom may be helpful to change this behavior. Affected young PBPs typically outgrow this condition. If water is restricted and offered only with meals, care must be taken to prevent salt toxicity.
3. Chronic kidney failure is a common cause of death in geriatric PBPs. Lethargy, anorexia, dehydration, azotemia, ammonia breath odor, and low temperature are possible presenting signs. Symptomatic treatment such as rehydration and antibiotics (procaine penicillin 22,000 IU/kg/day, IM, for 3 days) may be at least temporarily helpful in less severe cases.
Source: 9sites.org, merckmanuals.com, thepigsite.com
Gastritis and gastric foreign bodies are common in PBPs because they are omnivorous and prone to ingest many types of objects. Keeping PBPs indoors where they are unable to root and restricting calorie intake to prevent obesity probably contribute to this continual search for food. Dividing the daily ration into two or more portions and furnishing low-calorie foods (eg, lettuce, cabbage, celery, carrots, or green grasses) may help satisfy appetite. If an ingested foreign body is small or pliable enough, it may pass through the GI tract and cause mild gastritis that is self-limiting or only requires antibiotic therapy. Larger objects may remain in the stomach or partially pass into the duodenum or a more distal part of the small intestine. Clinical signs such as vomiting and colic can be acute but may be more subtle and increase in intensity over several days or weeks. Radiographs may reveal obvious foreign material or delayed gastric emptying. CBCs may indicate infection but are usually not informative; serum enzyme and electrolyte panels may only reflect dehydration. Surgical correction is indicated but may not be successful if extensive necrosis of GI tissue is present. Fluid replacement and nutritional supplementation plus antibacterial therapy and tetanus prophylaxis are indicated in convalescing PBPs
Lower GI obstruction due to bowel stricture occurs in geriatric PBPs. Anorexia, scant fecal production, and a bloated abdomen with massively distended intestines seen radiographically are typical. Sedation and endoscopic examination of the oral cavity, esophagus, and stomach are indicated to exclude other problems. Exploratory laparotomy and anastomosis with or without bowel resection is usually remedial.
1. Colibacillosis or Escherichia coli diarrhea is generally an important disease in young PBPs. Mortality may be high in piglets that have not ingested adequate colostrum in their first 24 hr of life. Older PBPs apparently develop resistance to colibacillosis. Diagnosis is through signalment, history, and fecal culture. Sanitation to minimize infective doses of pathogenic coliforms in the environment of young, nursing PBPs is important for prevention. Commercial swine vaccines to prevent colibacillosis are available but must be given to sows before farrowing to stimulate immunity and secretion of IgA into the milk. Treatment is based on in vitro antibacterial sensitivity testing, but antibiotics such as oral or injectable gentamicin or injectable ceftiofur are usually effective
2. Enterocolitis from Salmonella typhimurium infection can affect PBPs of any age, but it usually occurs after weaning. Sources of salmonellae include waste food from overturned garbage cans, exposure to carrier swine (such as the dam), or fecal material from other animal species. Mild to severe diarrhea with mucus and blood can result. Diagnosis is through signalment, history, and fecal culture or PCR. Salmonella spp are characteristically resistant to many antibiotics, so in vitro antibacterial sensitivity testing is important. Parenteral gentamicin at 2.2 mg/kg/day for 3 days may be effective in the interim. Untreated PBPs may die. Some recovered PBPs may develop rectal stricture after enterocolitis, resulting in megacolon and a distended abdomen. Subsequent straining to defecate can cause rectal prolapse. Surgical correction of the rectal prolapse will not correct the underlying problem. Owners should be advised that many Salmonella spp, including S typhimurium, are zoonotic. Healthy PBPs may be tested via fecal culture or PCR to determine their salmonella status. Multiple tests are more accurate predictors than single tests. Vaccines available for commercial swine have not been used much in PBPs.
Bacteremia or septicemia after S choleraesuis infection may also affect PBPs, usually after weaning. Sources of infection are similar to those of S typhimurium. Mild to inapparent diarrhea followed by fever, lethargy, anorexia, cyanosis of extremities, recumbency, and death may ensue. Diagnosis, treatment, prevention, and zoonotic potential are similar to those of S typhimurium; zoonosis is mainly a threat in immunocompromised people.
3. Constipation may be seen in PBPs; however, each normal bowel movement of a PBP is typically composed of one or more cylindrical formations made up of smaller, multiple fecal balls that may give the impression that the PBP is constipated. True constipation may occur due to low water intake in sedentary PBPs or to an actual disease. Careful evaluation is warranted before treatment is administered. Enemas may be contraindicated if there is pathology such as colitis. In simple constipation, fecal softeners or mild laxatives such as sodium sulfate or magnesium sulfate may be used. These should be given with food, if possible, because forced PO (by mouth) administration can result in aspiration pneumonia and death, especially with mineral oil. Encouraging increased water intake by flavoring with fruit juice or liquid gelatin may be helpful. Regular exercise is also beneficial to promote normal feces.
4. Rectal Prolapse This is a painful condition in which one or more layers of the rectum protrude through the anus. The prolapse may involve only one rectal membrane (incomplete) or all the layers of the rectum (complete). The condition is most frequently associated with a prolonged but ineffectual effort to empty the rectum. It is most common in young animals with severe diarrhea and some other lower intestinal tract conditions. Eating foreign objects may trigger this condition. Straining to urinate can also be accompanied by rectal prolapse, so obtaining a correct diagnosis is important. Your veterinarian can treat this condition surgically, and recovery is considered routine. Once your pig has had a rectal prolapse, the chances of it happening again are greater.
Rectal prolapse occurs due to straining from bowel irritation from diarrheal disease, rectal stricture after S typhimurium enterocolitis or previous rectal prolapse repair, cystitis or urolithiasis, persistent coughing, dystocia, or possibly genetic predisposition. Small, uncomplicated, recent rectal prolapses may be repaired via anesthesia and purse-string closure of the rectum that allows for minimal passage of feces. Larger, complicated prolapses require surgical excision. Recurrence is less likely after surgery but is possible regardless of method of repair.
5. Salmonella Infections Enterocolitis is an infection often caused by Salmonella typhimurium bacteria. Pigs can be infected at any age, but after weaning is most common. Sources of infection include waste food from overturned garbage cans, exposure to other pigs with the infection, and wastes from other animals. The signs include mild to severe diarrhea with mucus and blood showing in the fecal matter. Fever, lethargy or weakness, and a bluish or purplish discoloration of the legs, ears, and jowls may also occur. Diagnosis is made by testing your pig's feces for the bacteria. At the same time, your veterinarian will test the bacteria to determine which medication can best treat your pet's infection. Untreated pigs may die from the infection, so prompt veterinary treatment is important.
Salmonella choleraesuis bacteria may also cause infection. The signs are similar to those of S. typhimurium infection, described above. Again, early veterinary intervention and treatment is important as this infection can cause death.
All Salmonella infections should be treated carefully because the bacteria can easily infect humans. Be sure to wash hands carefully and thoroughly with a strong soap, especially when disposing of waste materials. Children should not be exposed to pigs with any Salmonella infection as they can easily be infected.
Integumentary System
1. Dry, flaky skin with minimal to severe pruritus is seen in virtually all PBPs. Wiping down the skin with wet towels each week will remove the flakes. Moisturizing lotions (eg, aloe vera) also temporarily alleviates this problem. Fatty acid supplementation can be used as a more longterm remedy, but caution must be exercised not to promote obesity.
2. Sarcoptic mange is the most important ectoparasitic disease of PBPs. Intense pruritus and dermatitis are the basis for a presumptive diagnosis. In many cases, the owners have pruritic skin lesions on the arms or abdomen. Examination of skin scrapings (deep enough to contain some blood) from several sites usually confirms the diagnosis in advanced cases but may be negative in less advanced cases if very few mites are present. In young PBPs, the source of infestation is usually the dam; in older PBPs, the source is usually other infested pigs. Young PBPs isolated from other pigs and kept as pets may harbor mange mites as a subclinical problem until mite populations increase sufficiently to make the condition obvious. Treatment with ivermectin (300 mcg/kg, SC, repeated in 2 wk) or doramectin (300 mcg/kg, IM, repeated in 3 wk), is indicated. Recently acquired young PBPs should be given a routine preventive injection of either parasiticide when first presented for examination.
3. Melanoma is an important skin tumor in swine. Tumor removal and evaluation of metastatic potential through histopathology is important for prognosis. Spontaneous regression of melanomas, with subsequent depigmentation of the hair, skin, and iris, is occasionally seen in PBPs; affected swine usually have normal life spans.
4. Sunburn may develop in PBPs exposed to sudden, high-intensity sunlight. Skin lesions may or may not be obvious, but affected PBPs appear painful and seem to have hindlimb weakness or paresis. A sunburned PBP may be “down in the back legs” and show intense pain with vocalization. A thorough history is important for the diagnosis. Exposure to further sunlight should be prevented. Symptomatic treatment is remedial.
5. Bleeding back syndrome (dippity pig syndrome) is of unknown etiology. Signs are almost identical to those of sunburn (pigs dip their backs, vocalize, and show signs of extreme pain) but with no history of sun exposure. Circular, serum-oozing lesions of various sizes are seen on lumbar skin surfaces. Affected PBPs recover in several days with restricted activity with or without symptomatic treatment. The condition may recur in some animals.
6. Erysipelas is an infectious disease caused by Erysipelothrix rhusiopathiae and is one of the oldest known diseases that affect growing and adult swine. Up to 50% of pigs in intensive swine production areas are considered to be colonized with E rhusiopathiae. The organism commonly resides in the tonsillar tissue; nonpathogenic species (E tonsillarum) have been described as residing in the tonsillar tissue also.
Disease outbreaks may be acute or chronic, and clinically inapparent infections are believed to occur. Acute outbreaks are characterized by sudden and unexpected deaths, febrile episodes, painful joints, and skin lesions that vary from generalized cyanosis to the often-described diamond skin (rhomboid urticaria) lesions. Chronic erysipelas tends to follow acute outbreaks and is characterized by low mortality, enlarged joints, lameness, and postmortem evidence of vegetative endocarditis. Pigs with valvular lesions may exhibit few clinical signs; however, when exerted physically they may show signs of respiratory distress and possibly succumb to the infection. (Please see the common disease section for additional information about Erysipelas)
(source: http://www.merckmanuals.com)
Musculoskeletal System
1. Lameness due to lower back, hindlimb, or forelimb weakness is common in PBPs. Because of their conformation, PBPs are susceptible to muscle pulls, ligament damage, and fractures of the back and limbs. Because PBPs usually struggle against manual restraint (predisposing to injury), sedation or anesthesia is often used for procedures such as prolonged examination, radiography, foot trimming, blood collection, and dental work. Tiletamine-zolazepam at 2.2 mg/kg body weight, IM (in the ham), provides excellent analgesia and chemical restraint for these minor procedures; recovery, although smooth, is prolonged and requires careful monitoring. Gas anesthesia is also used and has the advantage of rapid recovery time. Fasting for 24 hr and withholding water for 4–6 hr before sedation or anesthesia is recommended.
PBPs with injuries to the back or limbs are usually treated with anti-inflammatory drugs, such as buffered aspirin with antacid, flunixin meglumine, or glucocorticoids (eg, dexamethasone). Polysulfated glycosaminoglycan and/or glucosamine/chondroitin sulfate products may be tried in nonresponsive cases.
Fractures of the distal humerus and elbow area and femur are common. These occur from jumps off furniture (distal humerus), dog bites (elbow area), restraint (elbow area and femur), equine kicks (femur), and other trauma. Repair via pins, screws, plates, and external devices successfully restores some range of motion if fractures are immobilized properly and any sepsis is controlled
2. Infectious arthritis may affect the very young to older PBPs. Lameness with or without joint swelling in one or more limbs is the usual clinical finding. Erysipelothrix rhusiopathiae, Streptococcus spp, Mycoplasma hyosynoviae, M hyorhinis, Staphylococcus spp, and Haemophilus parasuis are possible causes. Treatment early in the disease course with an effective antimicrobial (eg, lincomycin at 11 mg/kg, bid for 3 days) may be effective. Treatment after chronic changes have occurred, antimicrobial ineffectiveness against the etiologic agent, or misdiagnosis are reasons for treatment failure and persistence of lameness. In chronic cases, pain management with anti-inflammatory drugs should be considered. Polyarthritis from neonatal infection of the navel may be due to various environmental bacteria, including Pseudomonas spp. If degenerative arthritis and joint fusion from chronic inflammation are present after polyarthritis, euthanasia may be warranted. Osteochondrosis may also be considered in shoulder, elbow, hip, and stifle lameness, but this condition is not common in slow-growing, light-muscled animals such as PBPs.
3. Overgrown and/or cracked hooves are a common cause of lameness. Regular exercise on abrasive surfaces (eg, concrete) will wear hoof ends and help keep them the appropriate length. In PBPs with overgrown, elongated hooves, normal yearly length can be maintained by routine yearly trimming under sedation or anesthesia. Hoof cracks can be caused by overgrown hooves. PBPs with cracked hooves may additionally require antiseptic cleaning with tamed iodine and systemic antimicrobial therapy (ceftiofur at 4.4 mg/kg/day for 3–10 days, or ampicillin at 11 mg/kg, PO, bid for 7–10 days).
4. Zygomycosis from Mucor spp infection has occurred in the distal hindlimb of a PBP. The large growth that encompassed the entire foot was composed of infected/abscessed tissue that involved bone. Amputation was remedial.
5. Tetanus may occur after wound contamination from dog bites, skin abrasions, oral cavity abrasions, or surgical procedures. Tetanus toxoid should be part of the routine vaccination schedule of PBPs at high risk of exposure. If there is no current tetanus toxoid vaccination, tetanus antitoxin (500–1,500 U, depending on body weight) should be administered IM in the neck after recovery from any surgery or dental procedure (eg, trimming of canine teeth). Treatment for tetanus is by massive doses of tetanus antitoxin and penicillin early in the disease, along with tranquilizers, isolation to minimize external stimuli, and supportive therapy.
6. Fractures Breaks in leg bones and back bones are common in potbellied pigs and require surgery. Implanted pins, screws, plates, and other devices can help restore motion and strengthen the affected bone(s). Providing an environment that does not encourage your pig to jump on furniture or higher surfaces is the best way to reduce the chance of broken bones. Stairs are a challenge for pigs, and providing ramps between the levels in your home is a good way to solve this problem. Please don't let your pig jump off of furniture, as this can lead to these kind of fractures.
Nervous System
1. Systemic bacterial infection can be caused by (in approximate decreasing order of importance) Streptococcus suis type 2, other Streptococcus spp, Salmonella choleraesuis, Haemophilus parasuis,Escherichia coli, other gram-negative bacteria, and Listeria monocytogenes. CNS signs may include fever, depression, incoordination, staggering, postural abnormality, head tilt, circling, nystagmus, seizures, and death. PBPs are most commonly affected from birth through 4–6 mo of age. Treatment with the appropriate antibacterial therapy (eg, extra-label florfenicol, which penetrates the blood/brain barrier) in the early stages of infection is most effective; however, death may be the first clinical sign. Because S suis type 2 is a zoonotic disease agent, care should be exercised to prevent human infection when performing necropsies on pigs dying from suspected CNS disease.
2. Overheated PBPs may be depressed, inactive, and recumbent and show open-mouth breathing or panting with an initial fever followed by a subnormal and decreasing temperature. The prognosis is grave, but some overheated PBPs may respond to resting on a cool surface and cooling only the head with water for 10–15 min followed by packing ice bags around the head. If the temperature is still not controlled, cold-water enemas can be used while additional areas of the skin surface are packed in ice. Symptomatic treatment is continued as indicated. You can try ice packs in the groin area and alcohol applied to the hooves. Wet wraps around the legs and cool wet cloths around the neck help as well.
3. Salt toxicity occurs after water deprivation for extended periods of time followed by sudden rehydration or, less commonly, after prolonged consumption of high-salt foods. Affected PBPs may have seizures, walk aimlessly, or show other CNS signs such as blindness or postural abnormalities. Diagnosis in the affected live animal is confirmed by high levels of serum sodium, usually 160–183 mEq/dL (normal range 142–153 mEq/dL). Gradual rehydration and symptomatic treatment to counteract cerebral edema is indicated, but severely affected PBPs may only be stabilized to a vegetative and blind status. The histopathologic finding of eosinophilic infiltration into brain tissue is also diagnostic.
4. Seizure from unknown cause occurs in PBPs.
Respiratory System
1. Atrophic Rhinitis This infectious disease of younger pigs initially causes sneezing, a runny or bloody nose, tearing, and distortion of the nose or snout. It is most often caused by Bordetella bronchiseptica and/or Pasteurella multocida, and less commonly by cytomegalovirus. It is usually transmitted from the mother to the piglet before weaning but can be transmitted from pig to pig after weaning. The more severe the rhinitis, the more likely it is that the pig's nose or snout will be permanently distorted. This distortion may become more pronounced as the pig grows.
Bleeding from the nose, with or without a crooked snout, is a common sign of the disease. Early treatment with antibiotics is recommended for acute cases. For pigs with chronic nose bleeds, cooling the area with cold water and keeping the pig calm are helpful. For pigs in dry climates, increasing the humidity of the air can offer some relief. Vaccines are available for atrophic rhinitis, but they must be used in pregnant mothers and unweaned pigs to be most effective. Watch newborn piglets for sneezing, nasal discharge, and tears. If these signs appear, your veterinarian should be consulted for prompt treatment.
2. Pneumonia can be a very serious disease in PBPs because of their relatively small lung capacity. The most common cause of pneumonia is from initial Mycoplasma hyopneumoniae infection, which immunocompromises the lungs, followed by Pasteurella multocida infection. Young pigs contract these infectious agents from their dams or from mixing with infected pigs after weaning. Antibiotic treatment may be more effective if directed against P multocida, because this bacterium becomes the most important pathogen once coughing is present for several days. Vaccines available for M hyopneumoniae in domestic commercial swine have been used in young PBPs to prevent mycoplasmal pneumonia and subsequent Pasteurella pneumonia. Vaccination in older PBPs is probably unnecessary unless risk of exposure warrants continued use.
Actinobacillus pleuropneumoniae causes a life-threatening pneumonia that may occur after infection from the sow or exposure to carrier animals. Signs range from coughing, fever, and lethargy to sudden death, depending on the serotype of A pleuropneumoniae. Prompt antibiotic treatment with penicillin or ceftiofur is indicated. Recovered PBPs usually have permanent tissue loss in affected lung areas and may have recurrent respiratory problems. Vaccines available for domestic commercial swine may be used in PBPs if there is an exposure risk.
3. Swine influenza (see Swine Influenza) is an important viral pneumonia in PBPs that are taken to fairs, exhibitions, and petting zoos and exposed to other pig populations. It is usually self-limiting after 7–10 days but can be fatal. H1N1, H3N2, H1N2, and H2N3 are the most common strains in domestic swine. Multivalent vaccines available for domestic swine could be used in PBPs if indicated. Swine influenza is a zoonotic disease.
Urinary System
1. Cystitis and urolithiasis are common in PBPs. Signs include frequent urination or straining to urinate. Urinalysis, urine culture, CBC, serum chemistry, radiography, and ultrasonography are important diagnostic aids. A sterile urine sample for culture can be obtained via cystocentesis. Cystitis without triple phosphate crystalluria should respond to extended antibacterial therapy based on in vitro sensitivity testing. Acidification of the urine may minimize recurrence of infection. Nephritis can occur after cystitis as an ascending infection. Leptospirosis may be a primary cause of nephritis. Increased BUN and creatinine values may aid in the diagnosis of nephritis and kidney failure. A 6-way vaccine for leptospirosis is routinely given to breeding PBPs (see Vaccinations) but may also be considered for routine use in rescue operations where many PBPs are housed in close contact. Vaccination may possibly reduce renal shedding of leptospires should PBPs become chronically infected and, therefore, minimize transmission of this zoonotic disease.
In a PBP that is straining and unable to urinate, the bladder size should be reduced immediately by cystocentesis after sedation and radiography (plain or contrast) or ultrasonography to evaluate the location of urethral and bladder stones. If the blockage is in the urethra, cystotomy is recommended (both sexes) to identify and remove calculi in all possible locations. Calculi in the urethra of males may be removed by cutting through the sheath to expose the distal penis, catheterizing the urethra, and backflushing into the bladder. Calculi that cannot be removed by this method must be surgically removed by incising the urethra at the location of the blockage. However, scar tissue at the healed incision may also cause urethral obstruction. Suturing of the urethra is followed by cystotomy and bladder flushing to minimize recurrence and then by inspection for more calculi. The bladder is then closed, and a Foley catheter is inserted into the bladder, tunneled through the abdominal muscles, and sutured to the skin. Several days later, the Foley catheter is occluded, and the urethra is inspected to determine patency and urine flow; if not patent, the Foley catheter is opened again, and the process is repeated several days later. When the urethra becomes patent, the Foley catheter is removed. Although the urethra in females is short, blockage can still occur. Because urethral catheterization is difficult without endoscopy, a Foley catheter is inserted into the vagina and inflated, and a purse-string suture is placed at the vulva. Retrograde flushing through the urethral opening in the vaginal floor is attempted. A cystotomy is then performed to remove all possible calculi, followed by routine closure of the bladder. Foley catheter placement into the bladder may not be necessary. Further treatment includes antibiotic therapy and acidification of the urine. Despite these efforts, some affected PBPs do not recover and require euthanasia. Perineal urethrostomies are usually only temporarily successful because the surgical site becomes occluded by amorphous material or urethral polyps, and patency cannot be reestablished. However, surgical methods have been described to correct failed perineal urethrostomies in PBPs. Rupture of the bladder is a grave complication because normal bladder tone may not return even after stones have been removed and the bladder has been surgically repaired. Laser lithotripsy has been used to fracture urethral calculi not removable by flushing.
2. Psychogenic water consumption should be considered in PBPs (especially young PBPs) with polydipsia and polyuria. PBPs may develop a habit of drinking water and urinating frequently because of possible boredom or unknown causes. Cystitis and crystalluria should be eliminated as differential diagnoses. Measuring urine specific gravity before and after a 12-hr water fast will demonstrate whether the affected PBP is able to concentrate urine. Ability to concentrate urine indicates normal kidney function and helps exclude diabetes insipidus. Estimating the daily water intake and urine output will further aid the diagnosis of psychogenic water intake or establish that water consumption and urination are, in fact, normal. Relieving boredom may be helpful to change this behavior. Affected young PBPs typically outgrow this condition. If water is restricted and offered only with meals, care must be taken to prevent salt toxicity.
3. Chronic kidney failure is a common cause of death in geriatric PBPs. Lethargy, anorexia, dehydration, azotemia, ammonia breath odor, and low temperature are possible presenting signs. Symptomatic treatment such as rehydration and antibiotics (procaine penicillin 22,000 IU/kg/day, IM, for 3 days) may be at least temporarily helpful in less severe cases.
Source: 9sites.org, merckmanuals.com, thepigsite.com
How To Give A Mini Pig An Injectable Medication:
Injections
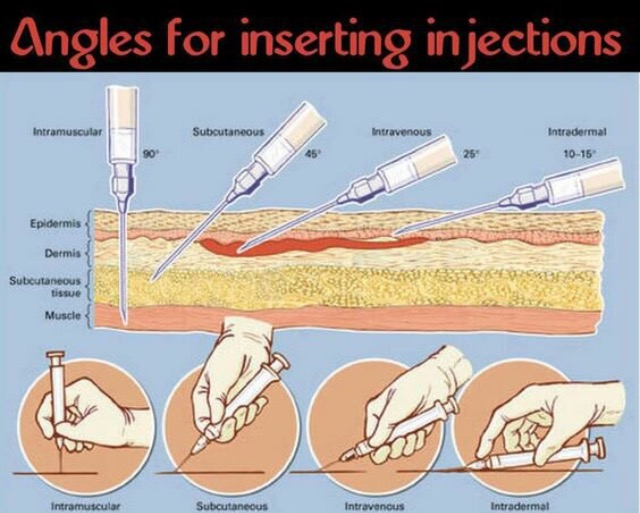
There are times when your vet will give you injectable medication for your sick pig. Injections are specific, some will need to be given IM (intramuscularly) some can be given SQ (subcutaneously-rare), etc. This diagram is how a needle will need to be positioned for each of the different types of injections.

Public Service Message
(From Lorelei Pulliam who has a pig rescue in northern Virginia)
One of their pigs was recently at the University of Tenn Vet Hospital with a blocked urethra. Because they got him there so quickly, (even though it is a 6.5 hour drive), he should recover. Most pigs suffer because their owners do not realize the gravity of the situation or it is misdiagnosed. This particular pig's bladder actually burst several years ago because a local vet misdiagnosed as constipation and sent home. His owner then abandoned him and left us with some very hefty bills.
Things every male pig owner should know:
- If you see your pig straining, you need to take immediate notice. It is often difficult to discern if they are trying to defecate or urinate. Some pigs will pump while standing there. They may still eat and drink.
- If no output, it is a red alert and they need immediate intervention.
- The surgery required will more than likely need to take place at a large vet hospital such as a University. Most local vets are not equipped to do so.
- A tube is placed into the bladder and out the abdomen for the urine to drain.
- The bladder will have a medication that breaks up stones flushed into it. This may take several days. They can also do a little roter rooter work in the urethra itself and look for stones and strictures.
- Once the urethra is open again, the tube is removed
- In the rare case that this does not work, a marsupialization can be performed with a permanent opening created for the bladder to drain. We had one elderly rescue live like this for several years after recurring blockages left no other option. He was 19 when it was done.
- Encourage your pigs to drink lots and pee often. One reason the stones form in the bladder is urine sitting too long. In my experience, it is usually house pigs that develop this condition.
- Recognize the symptoms, take quick action and know that there is treatment. It is a hard hard death if left unattended.
Routine urinalysis as part of an annual examination may enable early diagnosis and prevention of serious urinary tract disease in PBPs
(From Lorelei Pulliam who has a pig rescue in northern Virginia)
One of their pigs was recently at the University of Tenn Vet Hospital with a blocked urethra. Because they got him there so quickly, (even though it is a 6.5 hour drive), he should recover. Most pigs suffer because their owners do not realize the gravity of the situation or it is misdiagnosed. This particular pig's bladder actually burst several years ago because a local vet misdiagnosed as constipation and sent home. His owner then abandoned him and left us with some very hefty bills.
Things every male pig owner should know:
- If you see your pig straining, you need to take immediate notice. It is often difficult to discern if they are trying to defecate or urinate. Some pigs will pump while standing there. They may still eat and drink.
- If no output, it is a red alert and they need immediate intervention.
- The surgery required will more than likely need to take place at a large vet hospital such as a University. Most local vets are not equipped to do so.
- A tube is placed into the bladder and out the abdomen for the urine to drain.
- The bladder will have a medication that breaks up stones flushed into it. This may take several days. They can also do a little roter rooter work in the urethra itself and look for stones and strictures.
- Once the urethra is open again, the tube is removed
- In the rare case that this does not work, a marsupialization can be performed with a permanent opening created for the bladder to drain. We had one elderly rescue live like this for several years after recurring blockages left no other option. He was 19 when it was done.
- Encourage your pigs to drink lots and pee often. One reason the stones form in the bladder is urine sitting too long. In my experience, it is usually house pigs that develop this condition.
- Recognize the symptoms, take quick action and know that there is treatment. It is a hard hard death if left unattended.
Routine urinalysis as part of an annual examination may enable early diagnosis and prevention of serious urinary tract disease in PBPs
Prevention of urolithiasis in livestock (in general) by David C. Van Metre, DVM, DACVM downloadable file
| urolithiasis_prevention.doc |